Putting Barnsley people first...

When a child dies
When a child up to the age of 18 dies, there are certain processes that have to be followed to help us understand the reasons for the child's death, and enable us to address the possible needs of other children and family members in the household. Developing a better understanding of child deaths, and considering lessons we can learn from each case, helps us develop more effective prevention strategies for safeguarding children's welfare in the future.
The information below sets out the arrangements for a child death review across South Yorkshire which includes Barnsley, Doncaster, Rotherham and Sheffield.
All the information provided on this page is available to download in a single document Pdf. Click here to download.
Introduction
This document sets out how the Child Death Review partners and professionals in agencies across the four Local Authority areas in South Yorkshire will work together to review child deaths at a local level, and across the county of South Yorkshire, in order to identify learning that may help to prevent future child deaths. Across South Yorkshire there are approximately 100 child deaths per year and this will provide a larger cohort of data to enable better identification of themes, trends and learning.
The death of a child is a devastating loss that profoundly affects bereaved parents as well as siblings, grandparents, extended family, friends and professionals who were involved in caring for the child in any capacity. Families experiencing such a tragedy should be met with empathy and compassion. They need clear and sensitive communication. They also need to understand what happened to their child and know that people will learn from what happened.
The process of expertly reviewing all children’s deaths is grounded in deep respect for the rights of children and their families, with the intention of preventing future child deaths.
Definition
The Child Death Review process covers children; a child is defined as a person under 18 years of age. A child death review must be carried out for all children regardless of the cause of death.
This includes the death of any live-born baby where a death certificate has been issued. In the event that the birth is not attended by a healthcare professional, child death review partners may carry out initial enquiries to determine whether or not the baby was born alive. If these enquiries determine that the baby was born alive the death must be reviewed.
For the avoidance of doubt, it does not include stillbirths, late foetal loss, or terminations of pregnancy (of any gestation) carried out within the law.
- Stillbirth: baby born without signs of life after 24 weeks gestation
- Late foetal loss: where a pregnancy ends before 24 weeks gestation
Cases where there is a live birth after a planned termination of pregnancy carried out within the law are not subject to a child death review.
Principles
The process of expertly reviewing all children’s deaths is grounded in deep respect for the rights of children and their families, with the intention of preventing future child deaths.
The Child Death Overview Process within South Yorkshire will:
- Improve the experience of bereaved families, as well as professionals, after the death of a child.
- Ensure that information from the child death review process is systematically captured to enable local learning and, through the planned National Child Mortality Database, to identify learning at the national level, and inform changes in policy and practice.
Statutory requirement
The Child Death Review partners are local authorities and clinical commissioning groups for the local area as set out in the Children Act 2004 (the Act), as amended by the Children and Social Work Act 2017.
Working Together to Safeguard Children: A guide to inter-agency working to safeguard and promote the welfare of children (July 2018)
and
Child Death Review Statutory and Operational Guidance (England) (October 2018). These documents provide the statutory guidance for reviewing child deaths in England.
In addition, Working Together: transitional guidance also published in July 2018 provides for the transition to Child Death Review Partners in 2019.
Child death review partners
For the purposes of these arrangements, the responsible Child Death Review partners and the accountable officers in South Yorkshire are made up of the local authorities and clinical commissioning groups in Barnsley, Doncaster, Rotherham and Sheffield.
Statutory guidance
Implementing the key requirements from the statutory guidance:
Child Death Review partners within South Yorkshire will make arrangements to review all deaths of children normally resident in the local area and, if they consider it appropriate, for any non-resident child who has died in their area.Child Death Review partners within South Yorkshire will make arrangements for the analysis of information from all deaths reviewed.
The purpose of a review and/or analysis is to identify any matters relating to the death, or deaths, that are relevant to the welfare of children in the area or to public health and safety, and to consider whether action should be taken in relation to any matters identified. If Child the Death Review partners within South Yorkshire find action should be taken by a person or organisation, they will inform them. In addition, the Child Death Review partners will, at such times as they consider appropriate, prepare and publish reports on:
- what we have done as a result of the child death review arrangements in our area, and
- how effective the arrangements have been in practice;
- will request information from a person or organisation for the purposes of enabling or assisting the review and/or analysis process - the person or organisation must comply with the request, and if they do not, the child death review partners may take legal action to seek enforcement; and
- may make payments directly towards expenditure incurred in connection with arrangements made for child death reviews or analysis of information about deaths reviewed, or by contributing to a fund out of which payments may be made; and may provide staff, goods, services, accommodation or other resources to any person for purposes connected with the child death review or analysis process.
Key functions and responsibilities of local Child Death Overview Panels in Barnsley, Doncaster, Rotherham and Sheffield
The child death review partners for the local authority area in South Yorkshire where a child who has died was normally resident will be responsible for ensuring the death is reviewed. However, they may, in some circumstances, also choose to review the death of a child in their local area even if that child is not normally resident there. Child death review partners may wish to consider this for the deaths of looked-after children in their area who were not normally resident there. The review process will seek to involve child death review partners for another local authority area who had an interest in the child or any other person or agencies, as appropriate.
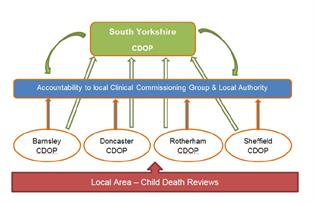
Each of the four local areas within South Yorkshire will retain local processes, Child Death Overview Panel (CDOP) and supporting pathways to review deaths of children who have died in and were normally resident in their area; and if they consider it appropriate the deaths of non-resident children who have died in their area.
Each local CDOP will be accountable to the local Child Death Review Partners in that area and arrangements for accountability and reporting will be decided at a local level.
The key function and responsibilities of each of the four local area CDOPs in South Yorkshire are to:
- collect and collate information about each child death, seeking relevant information from professionals and, where appropriate, family members;
- analyse the information obtained, including the report from the Child Death Review Meeting, in order to confirm or clarify the cause of death, to determine any contributory factors, and to identify learning arising from the child death review process that may prevent future child deaths;
- make recommendations to all relevant organisations where actions have been identified which may prevent future child deaths or promote the health, safety and wellbeing of children;
- notify the Child Safeguarding Practice Review Panel and their local Safeguarding Partners when it suspects that a child may have been abused or neglected;
- notify the Medical Examiner (once introduced) and the doctor who certified the cause of death, if it identifies any errors or deficiencies in an individual child's registered cause of death. Any correction to the child’s cause of death would only be made following an application for a formal correction;
- provide specified data to NHS Digital and then, once established, to the National Child Mortality Database; this will be undertaken via the eCDOP software system as used on a South Yorkshire wide basis;
- produce an annual report for the Child Death Review partners on local patterns and trends in child deaths, any lessons learnt and actions taken, and the effectiveness of the wider child death review process;
- provide data and analysis for the South Yorkshire Child Death Overview Panel to enable patterns, themes and trends to be analysed on a wider footprint to enable learning;
- contribute to local, regional and national initiatives to improve learning from child death reviews, including, where appropriate, approved research carried out within the requirements of data protection; and
- provide an annual report for the local Child Death Review Partners highlighting the effectiveness of the local child death review arrangements.
Membership of the local Child Death Overview Panels
Core representation of each of the local Child Death Overview Panel will ideally include: public health; the designated doctor for child deaths for the local area; children’s social care services; police; the designated doctor or nurse for safeguarding; primary care (GP or health visitor); nursing and/or midwifery; lay representation; and other professionals that child death review partners consider should be involved. However, it is for child death review partners at a local level to determine what representation they have in any structure reviewing child deaths.
Each local area will develop its CDOP Terms of Reference and local pathways to enable it to fulfil statutory guidance with regard to reviewing child deaths; and publish these within local safeguarding children procedures. The local pathways to support the child death review process should also cover the following:
- Immediate decision making and notifications.
- Investigation and information gathering.
- The child death review meeting
- Family engagement and bereavement support
Deaths in specific situations:
- Deaths overseas of children normally resident in England
- Children with learning disabilities
- Deaths of children in adult healthcare settings
- Suicide and self-harm
- Inpatient mental health settings
- Deaths in custody
Key functions and responsibilities of the South Yorkshire Child Death Overview Panel (CDOP)
The South Yorkshire Child Death Overview Panel will not review individual child deaths. Its purpose is to regularly review and analyse data and information about all child deaths (across the South Yorkshire footprint of approximately 100 to 120 child deaths per year) that have already had a local review undertaken. This will enable further analysis, identification of trends and learning to be gained, in order to prevent future child deaths. Each of the four areas in South Yorkshire have implemented the eCDOP system to enable more effective information sharing, data analysis across the county; and direct data link to the National Child Mortality Database.
Such arrangements will facilitate appropriate professional experts being present to inform discussions, and allow easier identification of themes when the number of deaths from a particular cause is small. By necessity themed panels will need to have access to more detailed but anonymised case information. In order to ensure the effectiveness of these discussions the level of information sharing should be proportionate but allow for meaningful analysis to take place.
In order to do this the South Yorkshire CDOP will:
- Adhere to the principles set out in Section 3 of this document.
- Hold themed discussions on a quarterly basis to review deaths from a particular cause or group of causes. This should provide an opportunity for greater understanding and shared learning.
- Enable any additional actions to be developed on a sub-regional basis region and resources and ideas pooled.
- Provide a forum where practice issues that have a regional impact can be discussed and taken forward collectively by the South Yorkshire Panel.
- Develop strategies, in conjunction with the four local CDOPs, with the aim of preventing future child deaths; this may include communicating with national bodies or those outside of the South Yorkshire area.
- Make recommendations to all relevant organisations where actions have been identified which may help to prevent future child deaths or promote the health, safety and wellbeing of children.
The arrangements for the conduct of the meetings will include the following:
- Chairing will take place on a rotational basis, drawn from the four local CDOP Chairs for the period of one year.
- Where necessary, a Deputy Chair will be arranged by the local area, who are currently hosting.
- The panel will meet for three hours on a quarterly basis, and be held in the area where the chair and business administration is being provided for that year.
- Provision will be made for ad hoc or extraordinary meetings as required.
Membership of South Yorkshire Child Death Overview Panel
The South Yorkshire CDOP is a multi-professional panel whose core membership may include senior representatives from the following agencies or roles:
- Public health
- Designated Doctor for child deaths
- Children’s Social Care Services
- South Yorkshire Police
- Bluebell Wood Children’s Hospice
- Safeguarding Health Practitioner
- Primary Care (GP or health visitor)
- Nursing and/or midwifery
- Lay representation
Additional professionals should be considered in relation to specific themes or specialist role, for example; coroner’s office, ambulance service or hospices.
In order for the meeting to be quorate, there must be at least one representative from each local authority, with a maximum of 4.
Administration of the Panel
Administration for the South Yorkshire CDOP will be provided from the same area as the incumbent chair though this will require the support and collaboration from the other local CDOP administrators.
Governance Arrangements
The terms of reference for South Yorkshire CDOP will be ratified by the respective Child Death Review Partners (CCG and Local Authority).
The Terms of reference will be reviewed annually.
A memorandum of understanding will be implemented between the Child Death Review Partners, which sets out how they will work together.
Reporting
A South Yorkshire CDOP annual report will be developed and published annually outlining the effectiveness of the South Yorkshire arrangements, including what lessons have been learned and actions taken to prevent future child deaths across the county. This report will be submitted to the local Child Death Review Partners.
Information Sharing and Management of Data
The South Yorkshire Child Death Review Arrangements will adhere to the Data Protection Act 2018 and the General Data Protection Regulations.
The eCDOP system which feeds local data directly into the National Child Mortality Database has undergone a Data Protection Impact Assessment.
The South Yorkshire Child Death Review Arrangements is a statutory partnership function, and is not a public authority for the purposes of the Freedom of Information Act 2000.
Transitional arrangements
The Child Death Review Arrangements at each local area level in South Yorkshire will adhere to the Working Together Transitional Guidance (July 2018) for the purposes of uncompleted child death reviews at the point of implementation of the new arrangements.